Robotic Radical Prostatectomy (RARP)
Procedures we perform
ABOUT ROBOTIC RADICAL PROSTATECTOMY
What is a robotic radical prostatectomy (RARP)?
Robotic radical prostatectomy (also know as robotic assisted radical prostatectomy)(RARP) is an operation to remove the prostate and seminal vesicles to treat prostate cancer.
It is performed using the da Vinci robotic surgical system.
Why is a robotic radical prostatectomy (RARP) required?
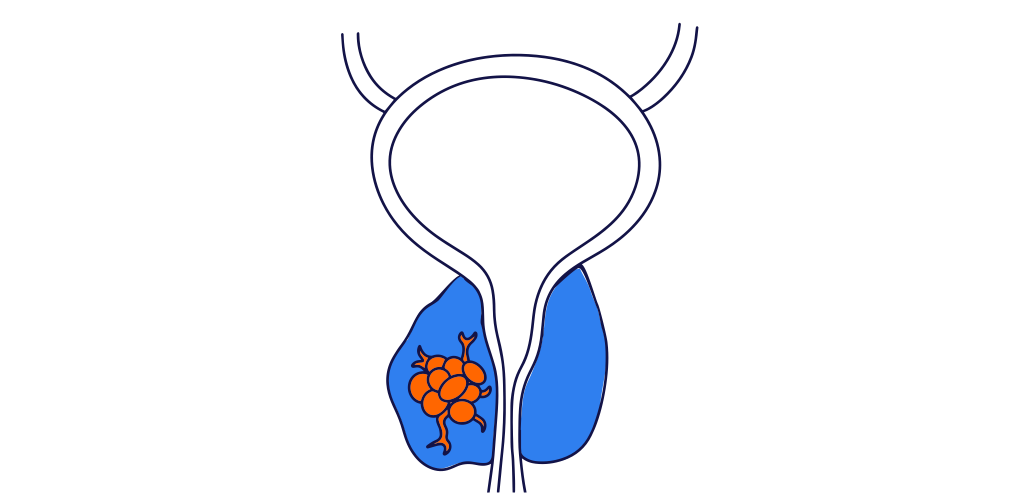
RARP is most commonly performed to treat prostate cancer which is localised to the prostate.
The aim of the operation is to cure the cancer, and to minimise the need for further cancer treatment, such as radiation therapy, hormone therapy, or chemotherapy.
RARP is occassionally performed for men with prostate cancer which has spread beyond the prostate (metastatic). In this case the aim of the operation is to control the cancer without curing it.
Read more about prostate cancer and PSA testing below.


PATIENT JOURNEY





OUR TEAM
Meet our Urologists
The following Urologists in our practice perform robotic radical prostatectomy:








