Orchidectomy
Procedures we perform
ABOUT ORCHIDECTOMY
What is an orchidectomy?
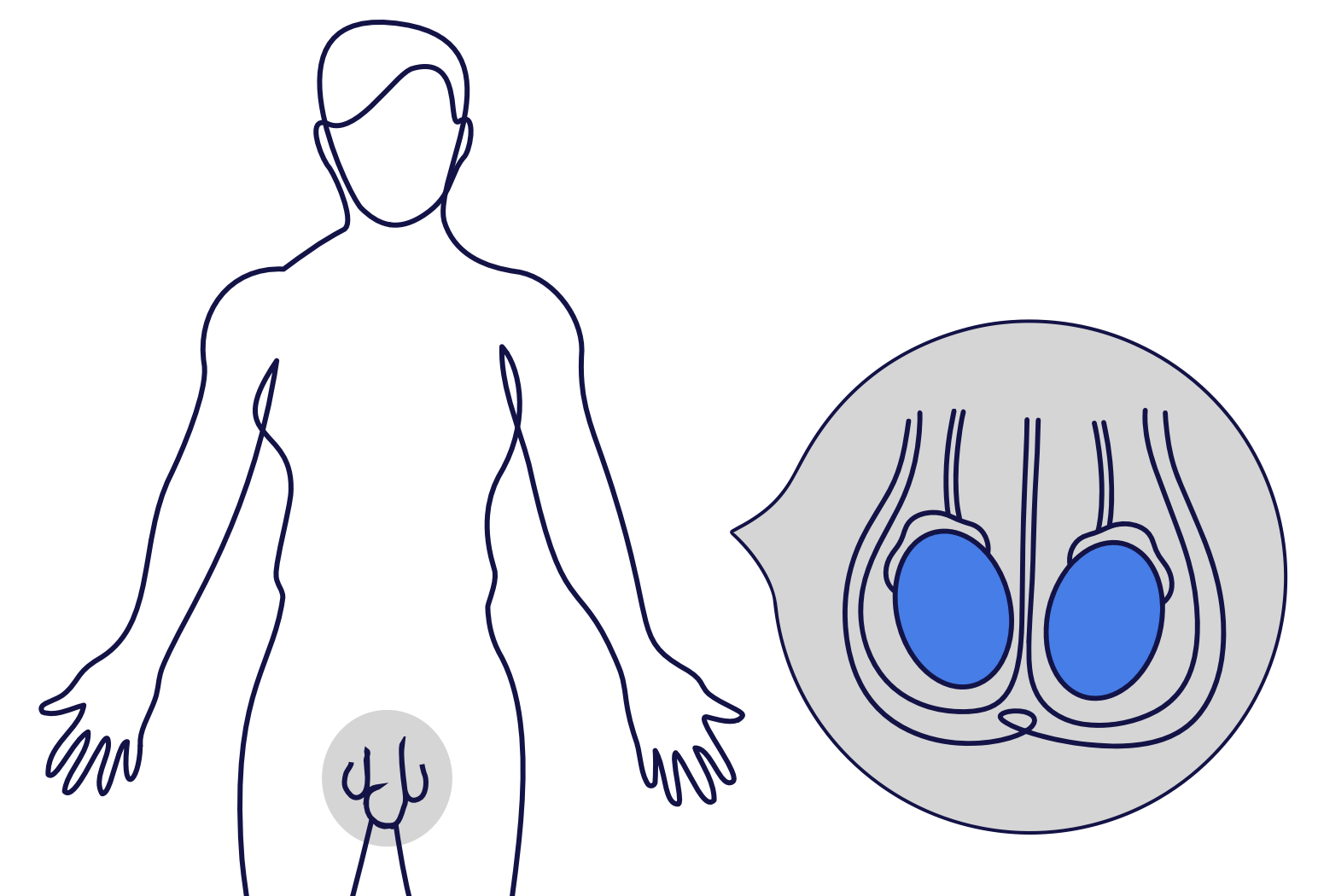
An orchidectomy (pronounced or·kuh·DECK·tuh·mee) is an operation to remove:
the testicle,
the epididymis (the sac on the back of the testicle which stores sperm), and
the spermatic cord (the cord that brings blood to and from the testicle).
It is also known as an orchiectomy, inguinal orchidectomy, or radical orchidectomy.
Why is an orchidectomy required?
Orchidectomy is most commonly performed to treat a mass in the testicle which is suspected to be a testicular cancer.
Occasionally, orchidectomy is performed to treat other conditions such as chronic pain, advanced prostate cancer, or severe infection which has spread from the urinary tract to the epididymis or testicle.
Read more about these conditions below.
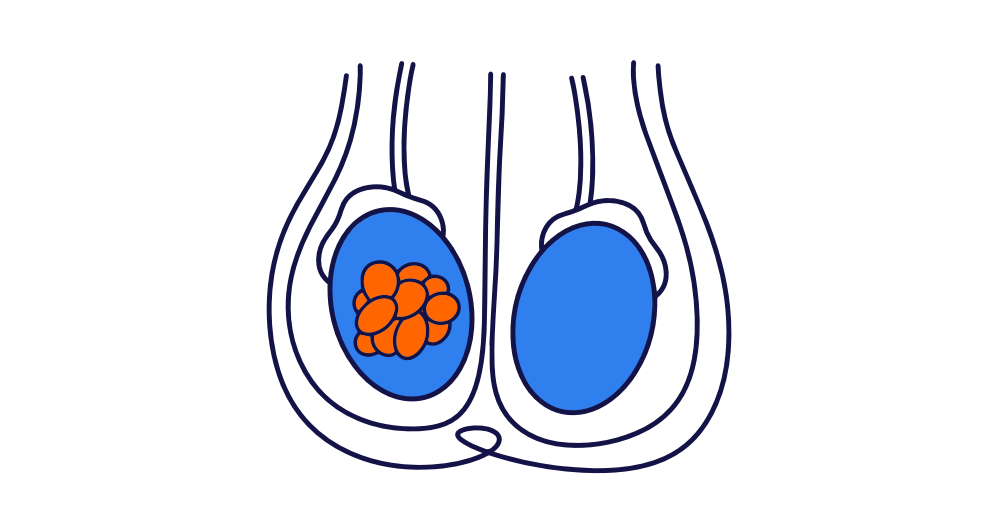

Testicular Cancer
Testicular cancer is a disease caused by the abnormal growth of cells in one or both testicles. These abnormal cells grow uncontrollably, forming a tumour, that can spread to other parts of the body.

PATIENT JOURNEY


OUR TEAM
Meet our Urologists
All of the Urologists in our practice perform orchidectomy.










