Holmium Laser Enucleation of the Prostate (HoLEP)
Procedures we perform
ABOUT HoLEP
What is a HoLEP?
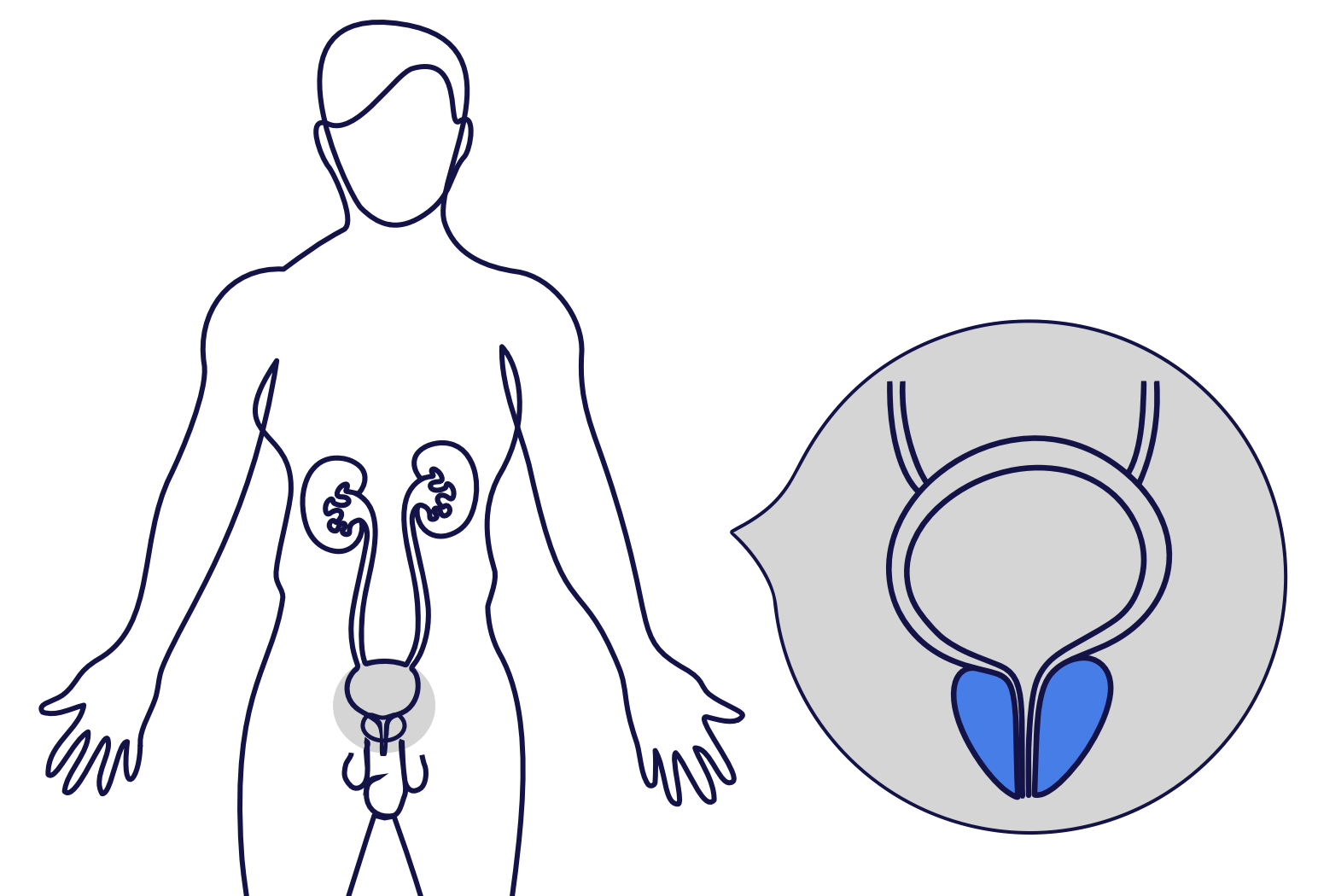
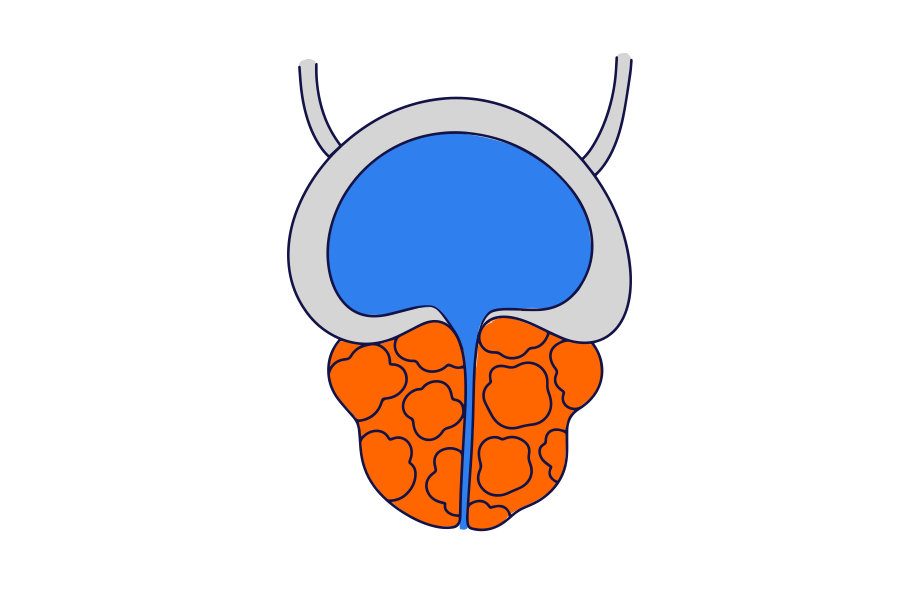
Holmium laser enucleation of the prostate (HoLEP) is an operation to remove prostate tissue which is blocking the flow of urine out of the bladder.
It uses a laser to remove the excess prostate tissue that is blocking urine flow.
HoLEP is effective for treating very large prostates and has a lower risk of bleeding than Transurethral Resection of the Prostate (TURP).
Why is HoLEP required?
HoLEP is usually performed to treat urinary symptoms due to benign enlargement of the prostate.
These symptoms may include:
Waking through the night to urinate.
Needing to pass urine frequently and urgently.
Reduced urine flow.
Difficulty starting urination.
Incomplete bladder emptying.
Read more about benign enlargement of the prostate below.

PATIENT JOURNEY


What are the alternative treatment options?
Our urologists offer a variety of surgical treatment options for the management of urinary symptoms due to prostate enlargement.
Read more about the alternative treatment options below.
Transurethral resection of the prostate (TURP)
Transurethral resection of the prostate (TURP) is a procedure used to treat urinary problems caused by an enlarged prostate.
Prostatic water vapour therapy (Rezūm)
Prostatic water vapour therapy (Rezūm) is a minimally invasive treatment for benign prostate enlargement. It uses water vapour to remove prostate tissue which is blocking the flow of urine out of the bladder.
Prostatic Urethral Lift (UroLift)
Prostatic urethral lift (UroLift) is a minimally invasive treatment for benign prostate enlargement. It involves placing implants into the prostate which retract the prostatic tissue.
Temporary Implanted Nitinol Device (iTIND)
Temporary implanted nitinol device (iTind) is a minimally procedure is a treatment for the management of an enlarged prostate. It involves placing a temporary implant into the prostate which reshapes the prostate.
OUR TEAM
Meet our Urologists
The following Urologists in our practice perform HoLEP:
